Home > Welcome > General medicine > Functional disorders > Chest and sleep > Chest and sleep
Chest pains are not often approached from the point of view of sleep but numerous situations of felt emergencies remain without a diagnosis while it is not considered.
According to common sense, the chest is the place where life sits. Any anomaly felt at that level has the value of an alarm sign and imposes a medical advice.
That opinion is totally shared by the emergency physicians for whom any pain located "between the head and the belt" imposes a transfer to the hospital within less than 3 hours.
Before anything else, it is necessary to consider the possibility of an illness which can show a life-threatening risk (infarctus, dissection or embolism) or require urgent care (pneumonia, pneumothorax ...).
Success of the treatment of these true emergencies depends on the speed with which they are taken care of and more and more sick people take advantage from it because of the emergency ambulance service (Samu in France).
In most cases, though, check-up is normal and the subject goes back home without any diagnosis.
In practice, that careful management of "felt emergencies" requires big means which are sometimes not relevant and takes a large part in the clustering of the emergency units.
![]()
«too many worries»
Mr T., 56 years old manager, is struck by a violent chest pain in the course of the evening and calls the ambulance according to his general practitioner’s advice. When he arrives, the characteristics and location of the pain (like being stabbed) do not give rise to much worry but his tension is slightly high and the ECG is not enough to rule out a cardiac emergency.
Out of caution, Mr T. is transferred to E.R. for a complementary check-up which reveals to be normal.
NB : The description of the pain (like a stranglehold), some hand positions (on the chest) rather evoke a coronary disorder to a doctor but there exist a lot more atypical pains.
In pratice, a blood check-up should be carried out in emergency in front of any unexplained pain of the chest : 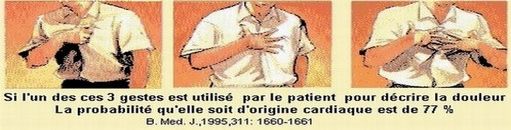
Later, we learn that Mr T. is in a great professional (under the threat of losing his job) and family distress (since his son died in an accident). He has no particular medical past history but he has already called the Samu twice this year : once for unbearable headaches (he thought he had an attack) and once for terrible colics (the doctors mentioned "gastroenteritis").
Mr T. strongly claims that he «sleeps very well» but admits that he wakes up very tired since two years (his wifes confirms). His doctor has even offered him an antidepressant treatment but he doesn’t take it...
«too much work»
Miss M is an independant physiotherapist and brings up her three children. She goes to E.R. twice for not very well defined pains which start to worry her. Relying upon her medical knowledge, she thinks it might be a cardiac problem but the doctors say that there is nothing wrong with her.
The cardiologist she sees downtown talks to her about "stress" and prescribes a long acting tranquillizer which causes the pain to disappear but Marie thinks that "she works too much and should be careful about that». She decides to limitate her professional and sportive activities. Later, she will see a doctor for insomnia and the diagnosis will be depression...
«no more time»
 Mr S. is a former high level sportsman (marathon) who has, since six months, a job of head-waiter in a big hotel. He calls a doctor on his work place for unbearable pains «in needle strokes near the heart» (he has already seen several cardiologists for that and no longer trusts their opinions). He admits that he has «no more time» to practice sport because he works too much.
Mr S. is a former high level sportsman (marathon) who has, since six months, a job of head-waiter in a big hotel. He calls a doctor on his work place for unbearable pains «in needle strokes near the heart» (he has already seen several cardiologists for that and no longer trusts their opinions). He admits that he has «no more time» to practice sport because he works too much.
The pain only disappears after a strong dose of injectable sedative...
The sudden stop of all sport (in intensive sportsmen or women) is the root of numerous functional disorders. The resumption of a regular sport is imperatively advised to prevent relapse.
![]()
Why move the emergency ambulance service?
It is always the level of fear which conditions the level of the aid :
- 1- postponed appointment
- 2- doctor on call
- 3- going to E.R.
- 4- call to the ambulance...
The fear, which is always the cause of the call, is not always in proportion with the seriousness of the chart.
Often, to the contrary, troubles caused by lesions are much less worrying than the felt emergencies (atypical precordial chest pains, «spasmophilia (or tetany)»).
- In the first case (lesional problem), the subject tries to comfort him/herself about the pain or sickness he/she feels : « Are you sure it is necessary to go to the hospital? It will go away, my wife, my neighbour, should not have called you.»
- In the second case (felt emergency), it is the fear linked to the feeling of imminent danger which comes to the foreground and the sick person feels the need to get closer to a place fitted with important means to manage to comfort him/herself : «Please hurry up! I’m not fine at all, I think you’ll arrive too late».
«Atypical precordia chest pains» (in other words, not lesional) are a part of the most frequent causes of emergency calls. The level of seriousness is zero but the pain is absolutely real.
In these three examples, the patient is in the situation of the «True False-sick. His/her worry is grounded on the potential seriousness of the sickness, but in the absence of objective criteria, the doctors consider that the fear is unfounded and that "the nerves" should rather be taken care of.
An interview that would focus on sleep would highlight a qualitative lack of sleep in each case but, very often, the subject notices no insomnia and turns his/her back to the true cause of his/her illness.
In the absence of any other diagnosis for these pains, it is tempting to point out "the nerves" or "stress" in front of that "anxious" sick person who "worries about nothing".
Yet, the embarrassment is real and, if the cause persists, the sick person will have no alternative but to keep on seeing doctors.
Unexplained chest pains are often simple signs of tiredness in a context of sleep inefficiency.
Some people’s sleep is very sensitive to states of hypervigilance. A subject who resists when facing difficult life events disturbs the quality of his/her sleep and tries to «stand fast» against the resulting sensation of tiredness.
It is the «vicious circle of tiredness and nerves». Functional disorders appear when that vicious circle reaches a stage of decompensation.
The somnological approach can offer a specific treatment.
In emergency, the treatment of the seizure relies on medications which «calm down» the nervous system. They are the only way to diminish the «noise of the alarm».
The success of this treatment is a good diagnosis test, in our opinion. Their unefficiency imposes to reconsider the situation and continue the check-up.
On a longer course, the caretaking of the underlying tiredness requires a deeper questioning about sleep hygiene and quality of living.
First, the patient must understand the link between the tiredness he/she feels, his/her unfitful sleep and his/her feeling sick.
He/she will have to find again a life rhythm which will suit better his/her personal resistance abilities.
![]()