Home > Welcome > General medicine > Functional disorders > Head and Sleep > Stiff neck
Introduction.
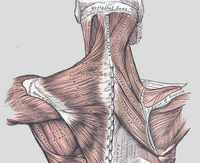
The neck is essentially made of a network of small muscles which work together in order to manage to support the skull’s weight (1 to 2 kg).
That synergy does not depend from will, there exists an automatic system which purpose is to harmonize those muscles’ contractions with the head’s movements.
Just like shrouds supporting a bridge, the system depends on a good distribution of the forces. In the context of the hypo-sleep syndrome, it all looks as though tiredness was combined with a loss of efficiency of that regulating system. One of the muscles gets out of synchronization with the others and induces a reflex contracture of the whole system.
A stiff neck is the painful freezing of some groups of muscles from the neck or the back linked to an often ordinary movement often described like an "awkward movement". The subject feels that "something has changed place" but the radiographs (which are generally useless here) do not show anything.

The stiff neck (like lumbago...) belongs to the set of functional disorders which appear in a context of overwork and/or tiredness.
The standard treatment relies on the combination of antalgic, anti-inflammatory treatments and (above all) rest.
Some physiotherapy techniques can reveal efficient like manipulations of the rachis meant to relax the contracted muscle.
If necessary, muscle relaxants can be used.
These "muscle relaxants" usually belong to the class of BZs (like Valium° or Diazepam), which all have a relaxing effect but present many unwanted side effects of sleepiness kind and memory loss (unlike it is thought, they have strong "anti-sleep" effects because they hinder slow deep sleep).
From a "somnological" Cf. neologisms for Smg point of view, we prefer to use some sleeping pills without BZs, considering that they can, exceptionally (one-off intake only), help to "strengthen sleep".

- The somnobar is in the red zone
In the context of tiredness resulting from an unefficient sleep (very different from insomnia), the subject becomes aware of the importance of sleep and uses the "sleeping pill" like a one-off tool in order to exit the system decompensation zone (Cf. "alarm system"). )
![]()
Example #1
Mr N. (41 years) consults in emergency room on a 15th of August for a severe stiff neck. He is worried because he had had to stop working for two month the year before at the same time of the year, "paralized" by pain. Besides, the scanner is normal and he doesn’t understand that "he can not be taken care of better".
- Emergency stop
The interview puts forward very atypical sleep schedules. Mr N. takes part in garbage removal and has to get up around 3 a.m. He goes to sleep later in the summer (the days are longer) and he has no more naps in order to be able to take advantage from his swimming pool.
He sleeps well, though, but "has no time". He admits he suffers regularly from "Excessive Daytime Sleepiness".
He is surprised (and a bit skeptical) to hear that sleep deprivation can be enough, in itself, to induce such a handicap.
![]()
Example #2
Mr G. has suffered from benign but repeated stiff neck (once a month in average) during several years. He thinks that pain comes from cervical arthrosis, which can be seen very well on the radiograph with its "beak shaped osteophytes". During that period he has, "besides", lot of troubles getting up in the mornings.
At 35 years of age, Mr G. already feels "like an old man" when he watches his radiographs.
Quite strange, though, ten years later, no more stiff neck... he no longer feels any pain, since he has changed his sleep rhythm. The arthrosis like on the radiographs is still there, of course, but since he wakes up easily, his muscles work fine.
Note : the axiom that there is "no correlation between radiograph and clinic" taught to the medicine students find, here, a perfect illustration.
![]()
Example #3
Ms B. calls for a «panic attack». She knows that disorder but, "since it doesn’t go away, she has to "bother a doctor" in case it was the heart or tension ..."
Here, we hear that, three years ago, she was hospitalized for a stiff neck that resisted every treatment. The surgeon wanted to operate her from a cervical hernia seen on the MRI, but she had refused and, finally, it had gone away.
Since then, she says she’s always tired (although she sleeps a lot...). On the other hand, she takes a lot of medications for arthrosis, blood circulation, memory, dizzy spells, heavy legs, tension, constipation and... she lacks magnesium (sic) !
Cf."False True-sick"
![]()
Discussion
In our experience, except for very exceptional (traumatic or infectious cases) cases, stiff neck is simply rooted in a somnological cause.
Here, whatever be the origin (sleep deprivation or a shift worker or hypo-sleep due to overwork, the occurence of a stiff neck is a sign of decompensation of the mechanisms of resistance. (Cf. "alarm system"). )
Stiff neck has the four common characteristics of the "Functional Disorders": it is worrying, capricious, disabling and is (fortunately) of a benign course.
It is a diabling (and sometimes desperating) disease but it always ends up healing spontaneously as soon as the subject recovers (with rest).
A few complementary thoughts:
1 : P ain appears at the occasion of a brisk movement while the subject is not aware of his/her level of tiredness. He/she is persuaded that his/her pain has a mechanical origin and lookds for a way to "unstuck" him/herself. That denial attitude towards tiredness is at the origin of often long, expensive, useless and sometimes dangerous (cervical hernia surgery) treatments).
As for Migraine or lumbago, it is striking to note that the subject is often unaware of his/her level of tiredness.
We call that phenomenon "deafness towards tiredness". The subject has a willing and resistant character and "refuses" to become aware that he/she is in the red zone (often because he/she has no other choice).
2 : Genders’ unequality in front of functional disorders is not chromosomic.
Unequality in front of house work is not either.
The hypo-sleep syndrome mostly reaches women and elder people because that population range is particularly exposed to the tiredness/resistance conflict.
The components of "Burnout" in a poorly recognized population of "workers" who can never get away from it are to be found there.
Conclusion:
The interview for a stiff neck must allow a good qualitative and quantitative estimation of sleep and put forward the other possible associated functional disorders.
Their presence in a context of tiredness when getting up points towards a "Hypo-sleep syndrome.
Relapse prevention relies on the application of correcting measures of sleep hygiene.
This pragmatic approach of functional stiff neck will not linger on the true reasons of overwork because, most often, the subject cannot get away from them.
In that context of helplessness and in the absence of "somnicological" guidelines, the sick person risks to enter the patients’ "assault course", in search for a diagnosis.
![]()

- More information...
- The site “Sleep and general medicine » is in continuous development, some updating may prove necessary in relation to the articles in French. As the site is in the process of being modified and completed, the translations into English have not been fully updated yet . Therefore, visiting the pages written in French for useful information is advised for the time being.
- The site is based on the collaborators’ voluntary involvement.
- If you wish to help us in this work, you are very welcome to participate. Do not hesitate to join in.
- Should you spot any mistakes or omissions, please do inform us.