Home > Welcome > General medicine > Chronic Fatigue Syndrome > Tiredness or sleepiness
Tiredness or sleepiness
Sunday 1 June 2008
To a good sleeper, the words for « tiredness » and sleepiness are synonyms, but, to a bad sleeper, they are very distinct sensations :
![]() Tiredness is constant with the insomniac subjet (it makes him/her want to sleep), but that feeling is not enough to induce sleep (on the contrary!).
Tiredness is constant with the insomniac subjet (it makes him/her want to sleep), but that feeling is not enough to induce sleep (on the contrary!).
![]() Sleepiness (the need for sleep) is the consequence of a sleep insufficiency (voluntary deprivation or linked to a pathology, like snoring).
Sleepiness (the need for sleep) is the consequence of a sleep insufficiency (voluntary deprivation or linked to a pathology, like snoring).
The nap (a very powerful "somnication") is very revealing of that difference. It is advocated for sleepy subjects while it should not be used at all in insomnia.
The caring of sleep disorders needs a clarification of the meaning of those two symptoms which the statistics on sleep do not always distinguish.
In the common language, media, and sometimes even in some scientific or medical articles, the words "tiredness" and "sleepiness" seem to cover the same meaning.
In practice, the caring of sleepiness is often diametrically opposed to that of fatigue. (The nap, for example, is indicated in sleepiness but is not to be used in tiredness because it leads to insomnia...)
The consequences of this misunderstanding are of four kinds:
- It favors « banalisation » of sleepiness and of the risks linked to the voluntary sleep deprivation;
- It leads to underestimate pathological snoring and delays the diagnosis of sleep apnoea;
- It favors and maintains the fears of the insomniac and leads to the vicious circle of sleeping pills;
- It contributes to hold the medical system in check on problems with fatigue and functional disorders. Such a lack of care for that type of sick people has a lot of costs and presents important iatrogenic risks.
Do «Tiredness » and « Sleepiness » share the same meaning ?
To a good sleeper, they are nearly synonymous...
- In the evening, when one feels « tired », he/she decides to go to sleep.
(Here, the common sense agrees to think that it is the same thing because going to bed will provide (the good sleeper) with the double satisfaction of getting rest and falling asleep whereas, under other circumstances, like getting on top of stairs, one can feel tired without feeling the need to sleep.)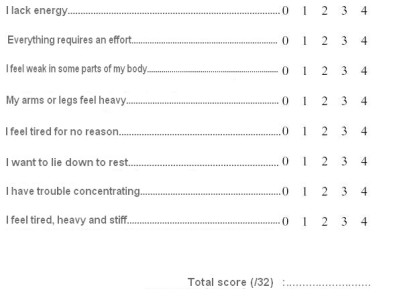
- Pichot scale of tiredness
- The teacher thinks that children who don’t get enough sleep are tired and have to go to bed early.
(Here, we don’t know whether the teacher is right or wrong. Does she speak about sleepy children who don’t get enough sleep because of the television, of the bigger children in the family, or about those who get up too early and who never feel the need to sleep in the evening ? It is striking to observe, on the contrary, that most insomniac children are fit during the day (be careful, it is at that early age that one learns (to fear) sleep.)
![]()
(Here, we assess the progress that still has to be made... Is it necessary to have a nap because of a feeling of tiredness or sleepiness ? The nap at work concerns, above all, the sleepy subjects, but it is not to be used in insomnia).
(We must keep in mind, here, that subjects with sleep apnea are (almost) always sleepy, (sometimes) tired but never insomniac because the micro-arousals all over the night increase the pressure of daytime sleep and not the opposite.
Nb. Insomnias linked to stress are, on the other hand, well endured during the day because they exert a stimulating and protective role on the subject in the situation of having to face a crisis. (The brain « on the war trail » physiologically doesn’t sleep much).
(Here, we assess the influence of the pharmaceutical companies that have financed the study. The deleterious role of napping in one case and its healing role in the other is overshadowed because the solution of insomnia appears, there, to be the key of sleepiness... ? All in all, it would be enough to take a sedative in order to avoid to be sleepy ?)
(Here, we observe the result of the mix-up between sleepiness and tiredness. One takes a sleeping pill the day before an exam, a sport trial, or in a plane to fight jet-lag. None of these attitudes rely on medically acceptable arguments but many doctors support that practice without assessing the short or long term risks.
(Advertisement plays on the fear of sleepiness to enforce the feeling of a person who lacks performance that he/she doesn’t sleep enough).
![]()
Screening of causes and consequences as well as care taking are though diametrically opposed
A/. Excessive daytime sleepiness (EDS)
- Screening:
A subject who suffers of excessive daytime sleepiness does not often consult spontaneously.
He/she has become used to fight the need to sleep (he/she yawns, drinks a cup of coffee) in daily life and chooses to have a short nap when the opportunity appears (in the train, on holidays, during the week-end). Since the media evoke the benefits of short naps, he/she agrees to think that he/she is a good sleeper because he/she falls asleep without difficulty in the evening.
The diagnosis is evoked in case of a score higher than 12/24 on the validated scale for sleepiness (Epworth) but certain subjects who score much higher are absolutely unaware of their state even if they fall asleep in a cinema, on a parking lot or while having a meal.Nb. This « silent » characteristic of EDS justifies the launch of systematic screening programs based on the model of that made against high blood pressure, for example.
The traffic accident linked to sleepiness is, in some ways, the equivalent of the cerebrovascular accident for the hypertensed person : one sees there is a problem but it is sometimes too late).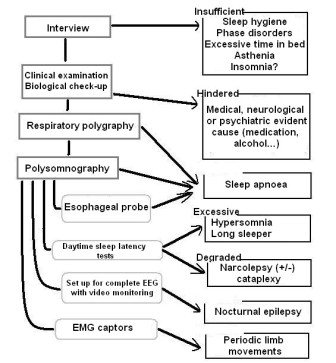
- Decisional tree for an excessive daytime sleepiness
- Causes:
EDS results of a quantitative lack of sleep of an exogenous or endogenous origin. The sleep doctors who are confronted to a problem of sleepiness follow an accurate decisional tree that leads to the diagnosis. (See the document).
The main causes of EDS are : voluntary sleep deprivation, sleeping pills and pathologic snoring. Other less frequent causes like idiopathic hypersomnia or narcolepsy are often diagnosed at the issue of an etiologic check-up (Cf.). - Consequences:
EDS is a mortal disease.
Statistics probably underestimate the part of excessive sleepiness in serious accidents. Apart from the risks linked to falling asleep, complex intellectual performances like taking decisions are very affected by EDS (this has been pointed out in the sequences of errors that lead to disasters like Tchernobyl) - Caretaking:
Apart from (preventive or curative) treatment of the cause, the nap is the best « somnication » to oppose to sleepiness. Yet be careful to know its user’s guide (See : the nap, indications of use and precautions)
Recent studies suggest that the reduction of performances (prejudicial to the company), that strike some of the workers around 3 PM, are reversible after a short nap on the workplace.
![]()
B/.Tiredness:
- Screening :
Tiredness can be screened during the interview of a subjects who consults for motives that go from functional disorders to asking for a tonic.
Pichot’ (cf.) scale of fatique allows to quickly estimate the intensity of the physical and intellectual handicap that the subject suffers of.
The nature of the 8 questions of which it is composed allows the patient to understand the difference better compared to sleepiness.
The functional disorders are defined by a very characteristic triad : they are worrying, capricious, resistant and of spontaneous healing without a known cause (migraine, colopathy, and many rheumatisms are typical examples).
Nb. This ambiguity between fatigue and sleepiness does not concern asthenia, which is the tiredness related to a lesional pathology (infection, heart failure...) nor psychasthenia related to depression (that marks itself out with its feelings of sadness, discouragement and self-depreciation that can lead, on the way, to the act of suicide).
Here, tiredness remains totally unexplained and strikes rather dynamic subjects, by sudden jolts, that force them to lay down or interrupt their activity.
We must listen to the terms used by the tired subjects to understand what they feel : « drained », « worn out », « knackered », and so on. It is the feeling of not being able to fulfill usual tasks without having to summon unexpected resources of willpower.
In the start, tiredness leads to rest and the subject is able to nap or go to sleep earlier. But that diminishes the « homeostatic » pressure of night sleep and does not contribute to bring the person the rest he/she seeks. - Causes:
In the absence of a known cause (normal check-up), tiredness could result from a disruption of the mechanisms that guarantee the efficiency of sleep.
Experimentally, the states of chronobiologic dissociations and jet-lag lead to very similar symptoms.
The advances of research on the Endocannabinoid System seem to strengthen the idea that there exists a system common to the center of regulation of all important functions of life.
That system would rule appetite, immunity, pain, mood and sleep...
According to our hypothesis, a disregulation of that system would lead to an unfulfilled need for sleep (like its action on appetite leads an obese person to want to go on eating without feeling satiety).
That insufficient sleep (« hypo-sleep ») would occur on a predisposed ground, on the occasion of difficult life events (of which the importance can be very variable).
Research on the genetic components of migraine or lumbago and sleep characteristics seem to strengthen the genetic hypothesis of fragility of sleep and pain components. - Consequences:
The consequences of fatigue are of three kinds :
- Economical : overconsumption of medication without benefit and cluttering up with limitation of access of the caretaking of lesional pathologies.
- Iatrogenic : The mortality and direct (linked to the examinations) and indirect (linked to the false-positives) morbidity, induced by functional disorders related to fatigue, is probably very important.
- Sociological : the failure of the bio-medical model in front of functional disorders has lead to a depreciation of the doctor-patient relationship that the initiatives of « health savings» will contribute to worsen (What shall we answer to an insisting demand for a scan by a person with chronic colopathy ?). - Caretaking :
As for obesity, the caretaking of fatigue is difficult and requires a « CBT » - cognitive and behavioral therapy - type approach adapted to each case.
It is important to obtain the support of the subject who must end up increasing his/her pressure of sleep by reducing his/her time of rest (which seems to him/her as paradoxical as to require from an obese subject that he/she must try to take on weight!).
Yet it is important to assess (with adapted tools) and to underline the aggravating role of sleep in the sensation of tiredness, migraine or stiff neck for example.
The « somnications » like light, sport, heat, or pleasure present synergic effects that oppose to tiredness.
In the absence of more efficient molecules, the SSRI (recommended in anxiety disorders like panic attacks) are sometimes used in this awakening strategy : « sleep less, sleep little, live better ».
![]()
A mix-up with heavy consequences.
- - Underestimations of sleepiness.
The advices that are in favor of napping at work do not take the causes of EDS into account and end up in an underestimation of sleep apnoea and other pathologic hypersomnias. - - « Banalisation » of sleepiness.
The sociologists underline the acceleration of rythms of living and problems of sleep deprivation inherent to modern society.
The nap, « controled and adapted to circumstances » could appear to be a precious asset in modern life management, but banalisation of the excessive daytime sleepiness can contribute to underestimate the importance of sleep.
That mix-up around the nap (chosen or not... ) is at the root of a bad communication.
For example, we know that the advices of « Bison Futé » (a French radio station dedicated to the drivers) have revealed to be dangerous because the drivers overestimated their performances when facing sleep deprivation before driving a vehicle.
We know that the drivers who volunteer not to drink in parties and discotheques are not aware of the risks that exist to drive a car around 3 or 5 AM, the period of the 24 h cycle that has been named « The compulsory gate to sleep » by the specialists.
Those young people are never told that sleepiness is sometimes more dangerous than alcohol and the surveys do not take the problems of sleepiness into account. - Cluttering up of the exploration units by patients who suffer of fatigue.
The media hype on sleep disorders and the mix-up between the complaints of sleepiness and fatigue lead numerous tired subjects to consult for sleepiness.
This misunderstanding leads to a cluttering up of the sleep exploration units that can only confirm the absence of effective sleepiness and let somebody else get away with it. - Bad estimation of the complaint of tiredness.
Tiredness is a frequent complaint in general medicine. It can be the common denominator between functional disorders as varied as migraine or allodynia, spasmophilia or fibromyalgia...
At the first stages of fatigue, the subject presents numerous functional disorders but he/she is able to sleep « a lot » and sleep is not at the center of his/her concerns, meanwhile, he/she admits that he/she complains of unexplained tiredness.
Subsequently, tiredness leads to a spiral of visits to the doctors and check-ups that thwart the medical approach. The sick person is brought to question the reality of his/her symptoms.
Those patients whom some have called « homeless » of medicine often find themselves confronted to the helplessness of the medical profession and are ready for anything rather than sink into despair.
That behaviour is at the root of unjustified expenses and presents numerous iatrogenic risks.
Yet, in the absence of a satisfying caretaking, the complaint of fatigue gets more and more chronic. - Favoring insomnia.
Tiredness is the engine of insomnia.
The medical history of an insomniac subject is punctuated by periods of tiredness and functional disorders that form, gradually, the certainty that he/she has to manage to sleep.
Thus, he/she behaves like a subject who follows a too strict diet and tries to take control over his/her feeling of hunger. The failure results in a rebound of weight gain.
The tired subject tries to take the control over falling asleep (which is a very natural sensation for a fit subject) and the failure results in rebounds of occasional insomnias. - Aggravating insomnia
The problem of the insomniac subject is totally centered on that of tiredness.
Insomnia only exists because the subject is tired (sometimes since a very long time) and he/she attaches more and more importance to sleep.
The subject who suffers of fatigue has transformed the need to sleep in willing to sleep.
Insomnia appears at the stage when the sick person completely looses the control on his/her sleep.
The mix-up between the problems of fatigue, insomnia and sleepiness leads to an occasional « on demand » consumption of sleeping pills by a subject who thereby looses faith in his/her sleep.
The problem of insomnia appears as soon as the product acts no more. It is the stage where a syndrome of withdrawal will block out any poorly coached attempt to stop.
The vicious circle of the sleeping pills reinforces, in this way, the vicious circle of insomnia.
![]()
Conclusion
Sleep medicine is still very young and lacks accuracy in the definition of these concepts.
It is important to be able to distinguish well the differences that oppose the complaint of sleepiness and that of tiredness because the taking care of those symptoms are not of the same kind.
- It can even favour a better screening of the sleepy subjects.
- It can offer a better quality of life to the tired subjects by offering them a new therapeutic way.
This lighting contributes to call into question the use of sleeping pills in the care of (even occasional) insomnia to the advantage of « somnication ».
These natural sleep medications take elements of chronobiology into account, which are light, heat, pleasure, laughter and love.
We know phototherapy, chromotherapy (filtering glasses), thermotherapy, musictherapy and even laughingtherapy.
Love has not, until now, been the object of validated studies but its beneficial effect as much on tiredness as on sleepiness is wellknown. Unfortunately, it is not possible to prescribe it.
This distinction is essential for the caring of insomnia.
Rabelais had noticed that « the cheerful recover quickly », but we think that it is more right to say that the « cheerful » do not suffer of any of the functional disorders that are linked to tiredness or sleepiness, and fill our waiting rooms.
![]()